

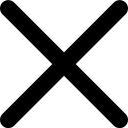


Why BPC-157 Capsules Don’t work the way people expect
BPC-157 capsules underperform because the peptide is largely blocked and degraded in the gut, so very little reaches the bloodstream in an intact, active form, especially compared with routes that bypass digestion. Delivery systems that keep BPC-157 out of the gastrointestinal tract and in contact with absorptive mucosal surfaces are far better aligned with how peptides actually move through the body.
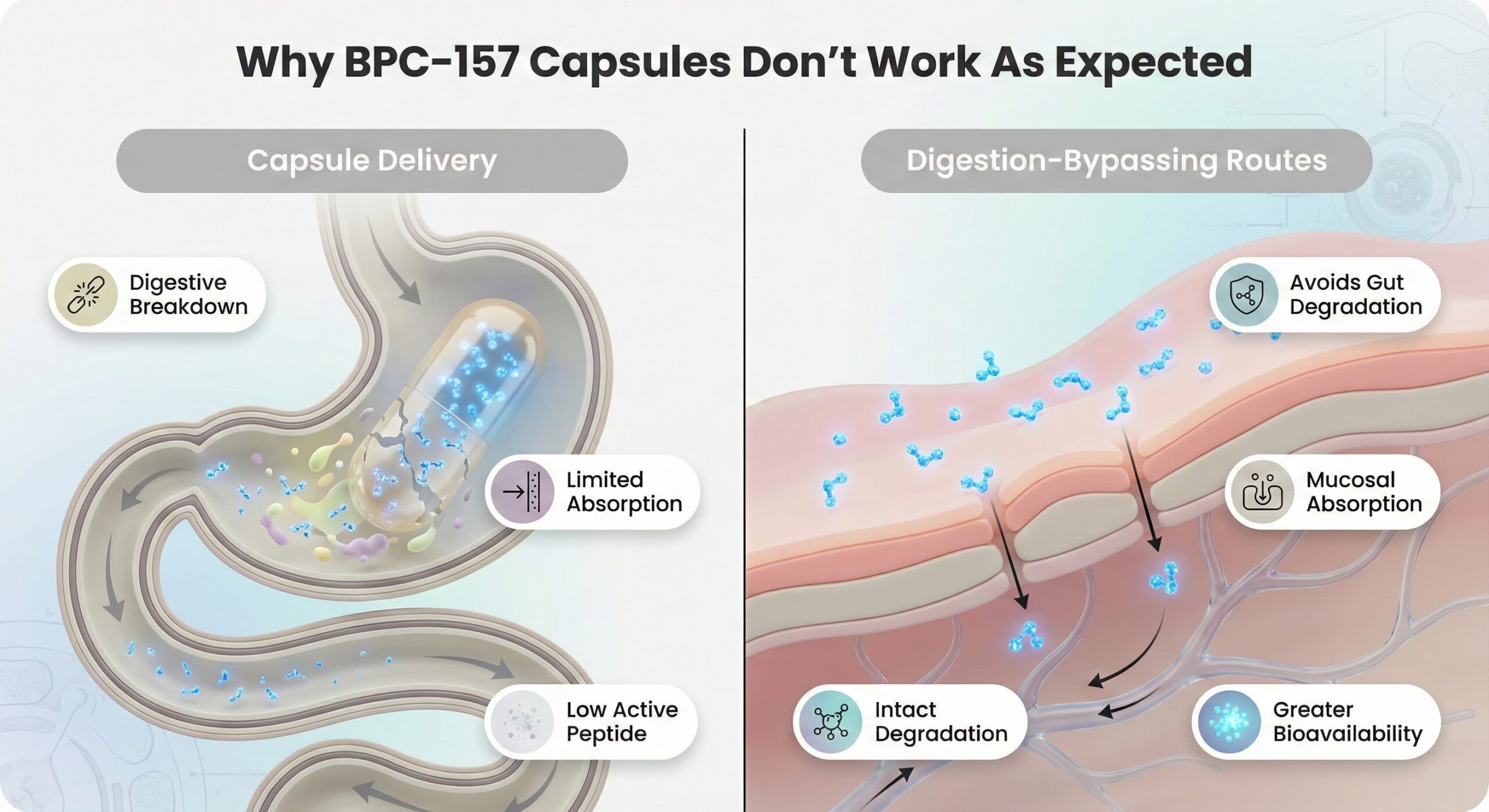
Why Capsules Fall Short
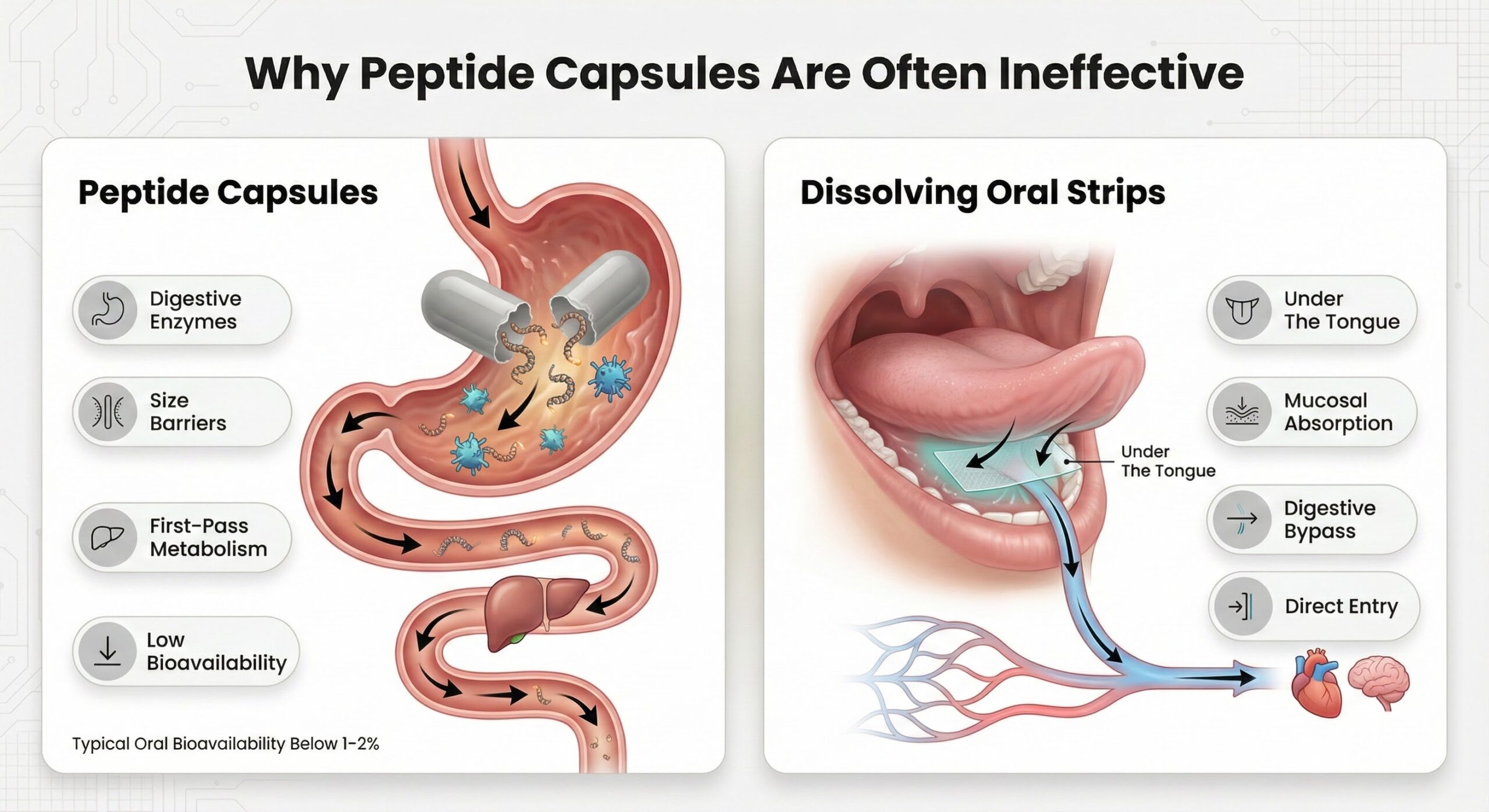
Capsules drop BPC-157 directly into the digestive tract, where it encounters enzymes designed to break peptides into amino acids long before they can act as signaling molecules. Even though BPC-157 is unusually stable in gastric juice, that stability does not solve the core issue that intact peptide must still cross the intestinal wall in meaningful amounts to have systemic effects.
The intestinal barrier is built to keep large, water-loving molecules out, favoring very small or specially transported compounds instead. As a result, oral peptide bioavailability is often at or below the low single digits, which is rarely sufficient for the systemic healing outcomes people expect from BPC-157 capsules.
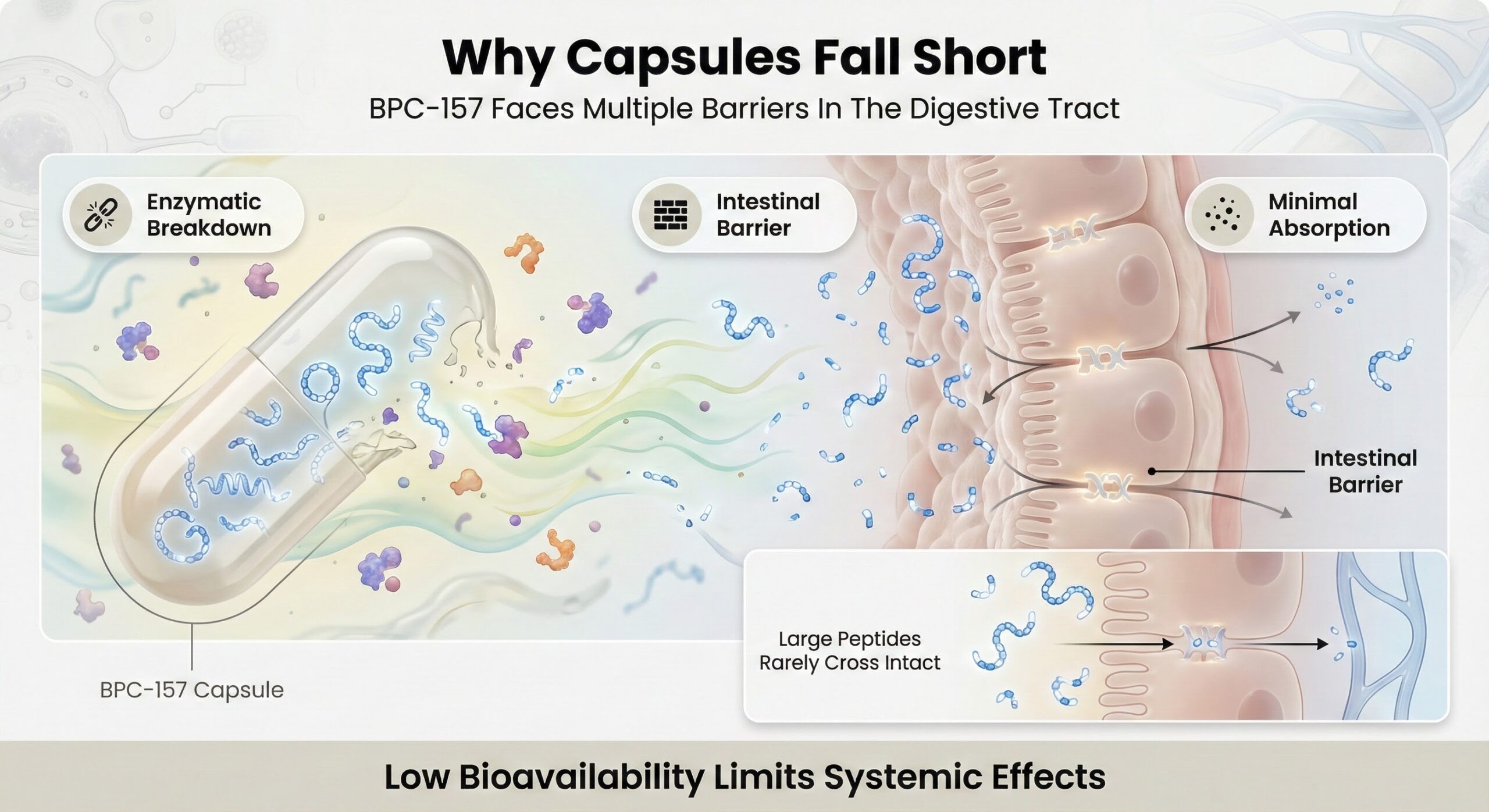
Barriers Inside The Gut
Multiple layers in the gut work together to limit peptide uptake. A mucus layer and tightly joined epithelial cells form a selective filter, making it difficult for mid-sized peptides to reach circulation intact. At the same time, pancreatic enzymes and peptidases continually cleave peptide bonds, channeling BPC-157 fragments into normal protein metabolism rather than targeted repair.
Changes in pH from stomach to small intestine further stress peptide structure and favor breakdown over absorption. For a capsule to deliver systemic benefit, the peptide would need to survive this environment and then cross a barrier that is inherently resistant to molecules of this size and chemistry.
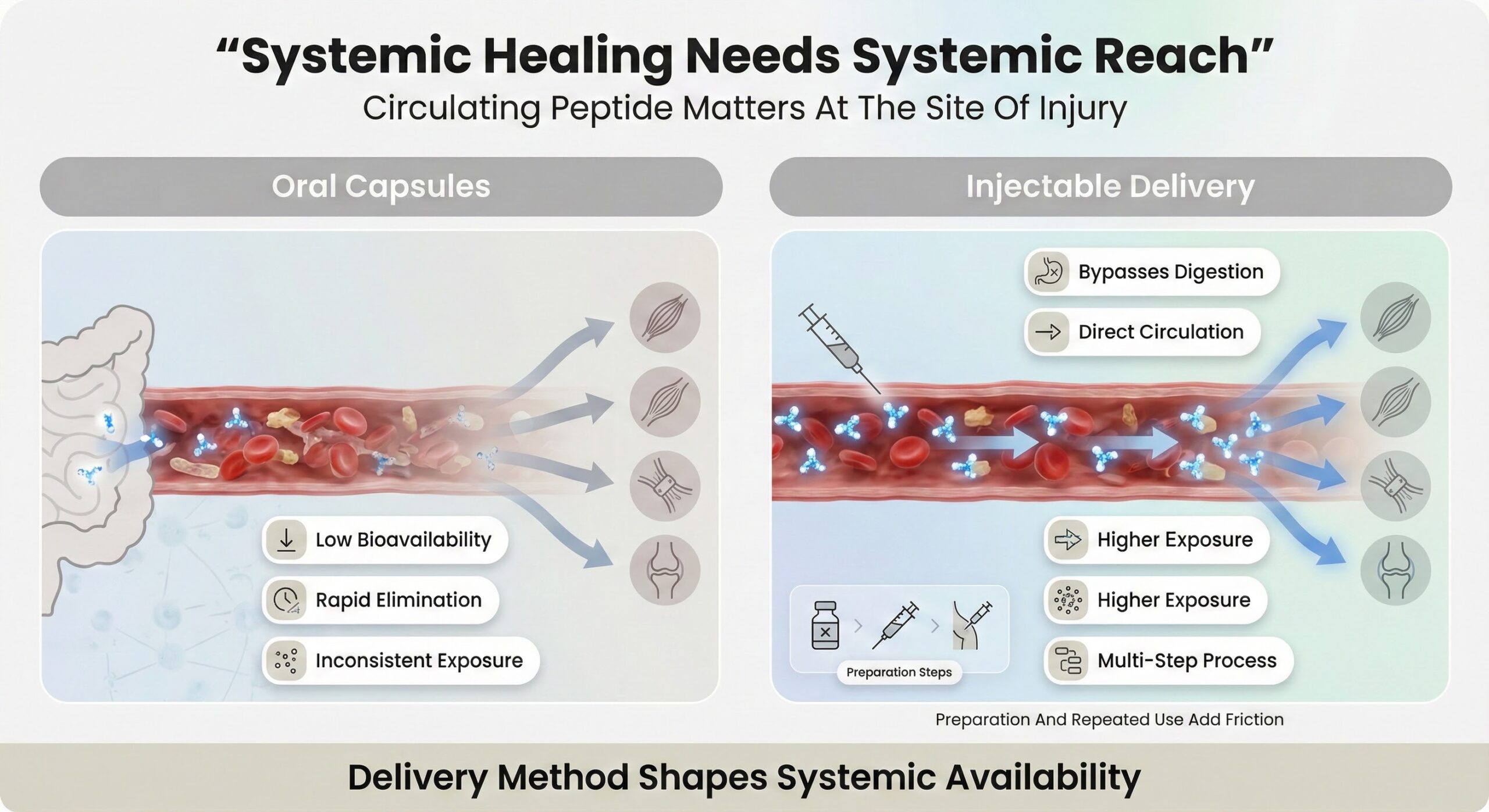
Systemic Healing Needs Systemic Reach
Muscle, tendon, ligament, and joint support depend on active peptide circulating at the site of injury, not just passing through the gut. When oral bioavailability is low and elimination is relatively rapid, the window during which enough intact peptide is present in blood and tissues becomes narrow and inconsistent.[1]
Injectables avoid the digestive system completely and can deliver BPC-157 directly into systemic circulation or near target tissues, which is why they are often considered the most straightforward way to achieve systemic exposure. However, they also function as a multi-step system that requires reconstitution, sterile technique, accurate measurement, and repeated injections—each step adding friction, user error potential, and psychological resistance over time.
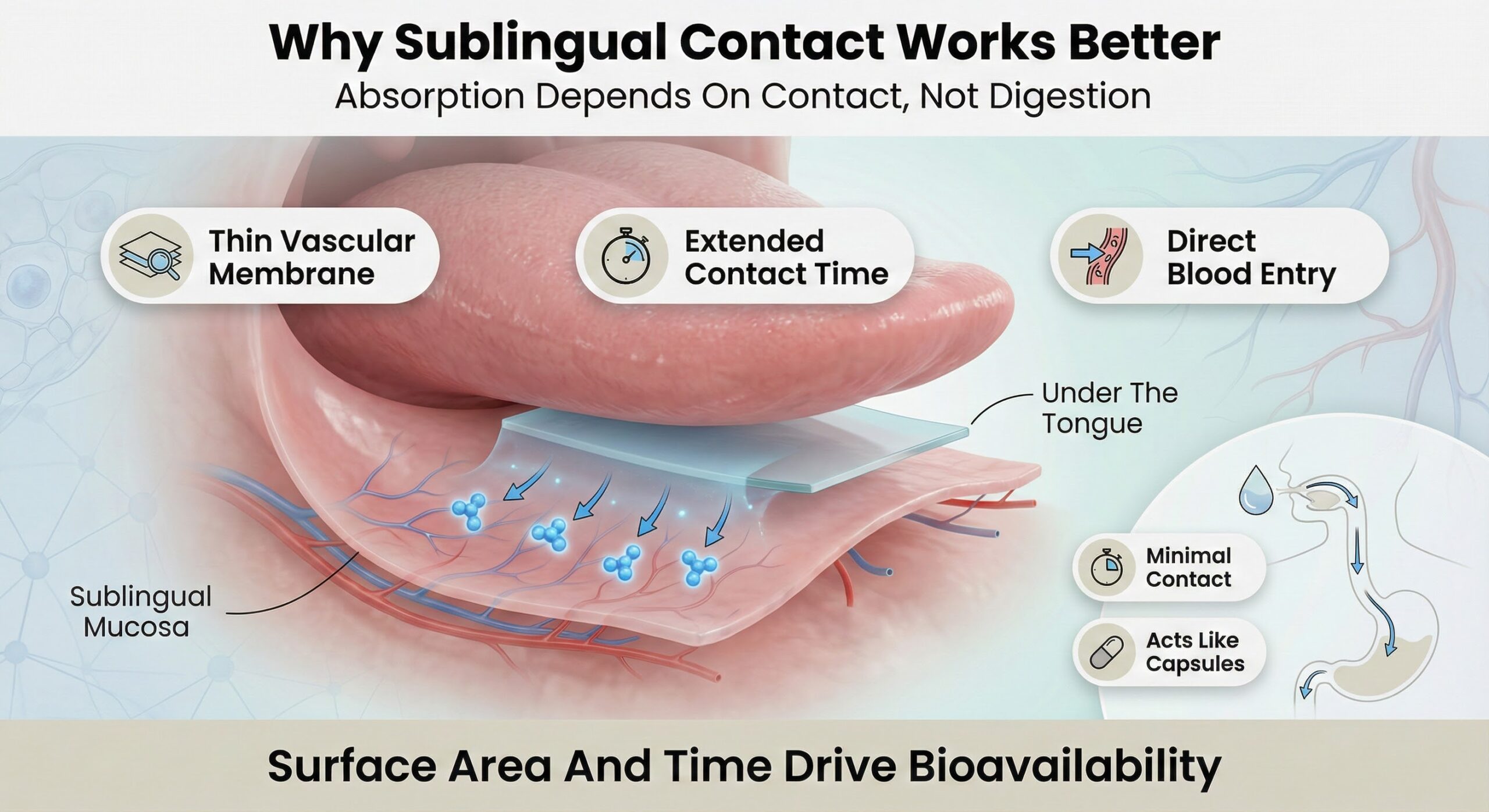
Why Sublingual Contact Works Better
Sublingual delivery exploits a thin, highly vascular membrane under the tongue that allows small molecules and certain peptides to enter the bloodstream directly, bypassing the gastrointestinal tract and first-pass liver metabolism. In peptide research broadly, sublingual administration has shown higher bioavailability than swallowed oral routes, with some models reporting upticks from roughly low single digits to clearly higher percentages.
Keeping a peptide in close contact with oral mucosa is critical, because absorption depends on surface area and contact time rather than surviving digestive fluids. This is why simple oral liquids that are swallowed quickly tend to behave more like capsules than like true sublingual systems; the peptide spends little controlled time on the mucosal surface before being swept into the gut.
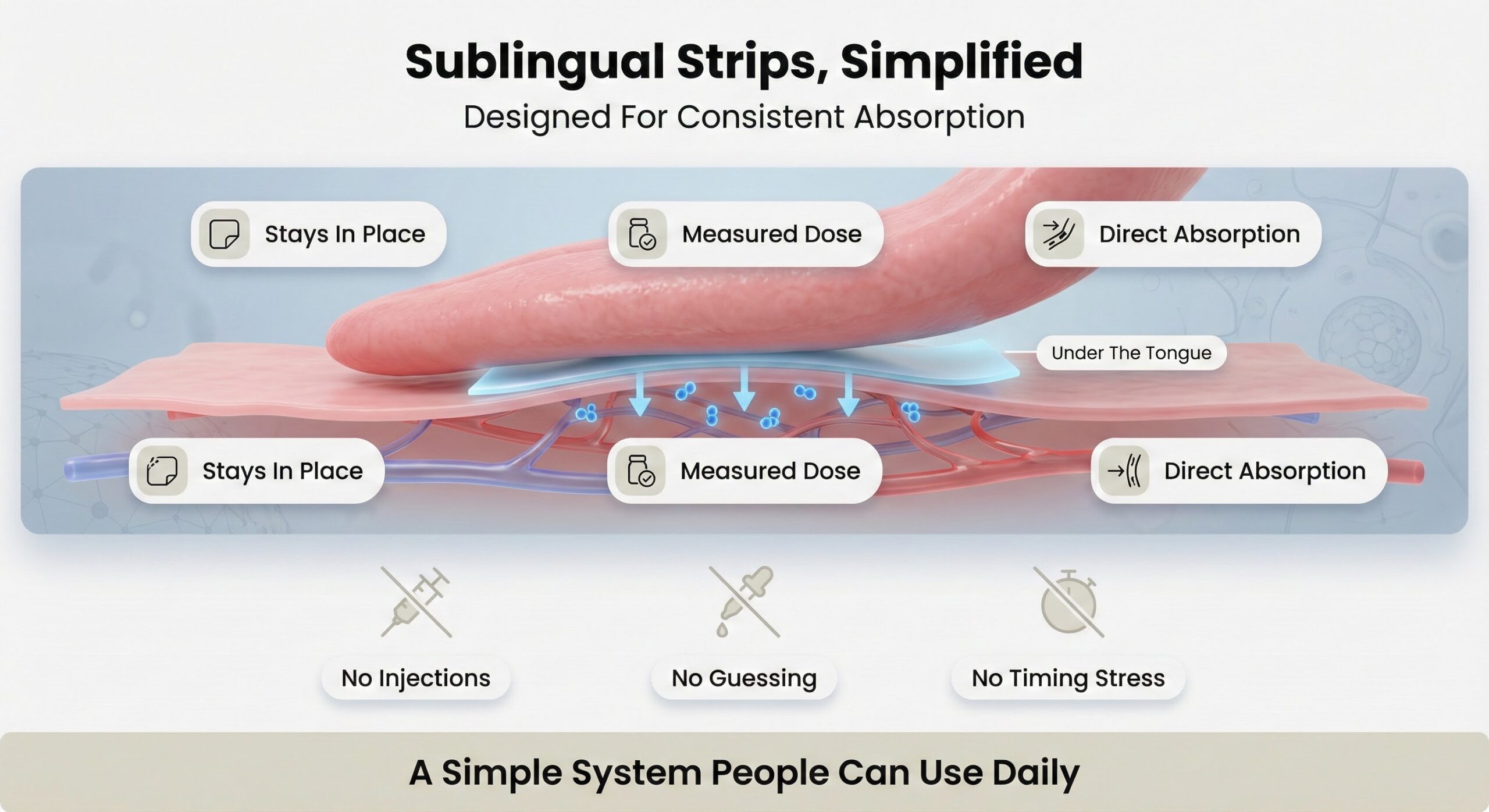
Strips As A Practical Daily System
Dissolving oral strips are engineered to sit on the oral mucosa and release a precise, pre-measured peptide dose as they dissolve, keeping the compound exactly where sublingual absorption can occur. Because the strip adheres and then disappears, there is no need to manage timing, avoid swallowing too early, or guess whether enough contact time has elapsed on a given day.
This single-step format removes many of the failure points present in injections and free-pour liquids—no reconstitution, no syringes, no volume calculations, and no risk that the dose ends up in the stomach instead of across the mucosa. By combining direct mucosal contact with built-in dose accuracy, strips make it far more realistic for someone to use BPC-157 consistently enough for its pro-healing mechanisms—support of blood flow, modulation of inflammation, and growth-factor signaling—to matter in real-world recovery. [1]
References
- Vasireddi N et al. "Emerging Use of BPC-157 in Orthopaedic Sports Medicine: A Systematic Review." HSS J. 2025. [View Study]
Read More

Preventing Overuse Injuries: The Role of Recovery
March 11, 2026
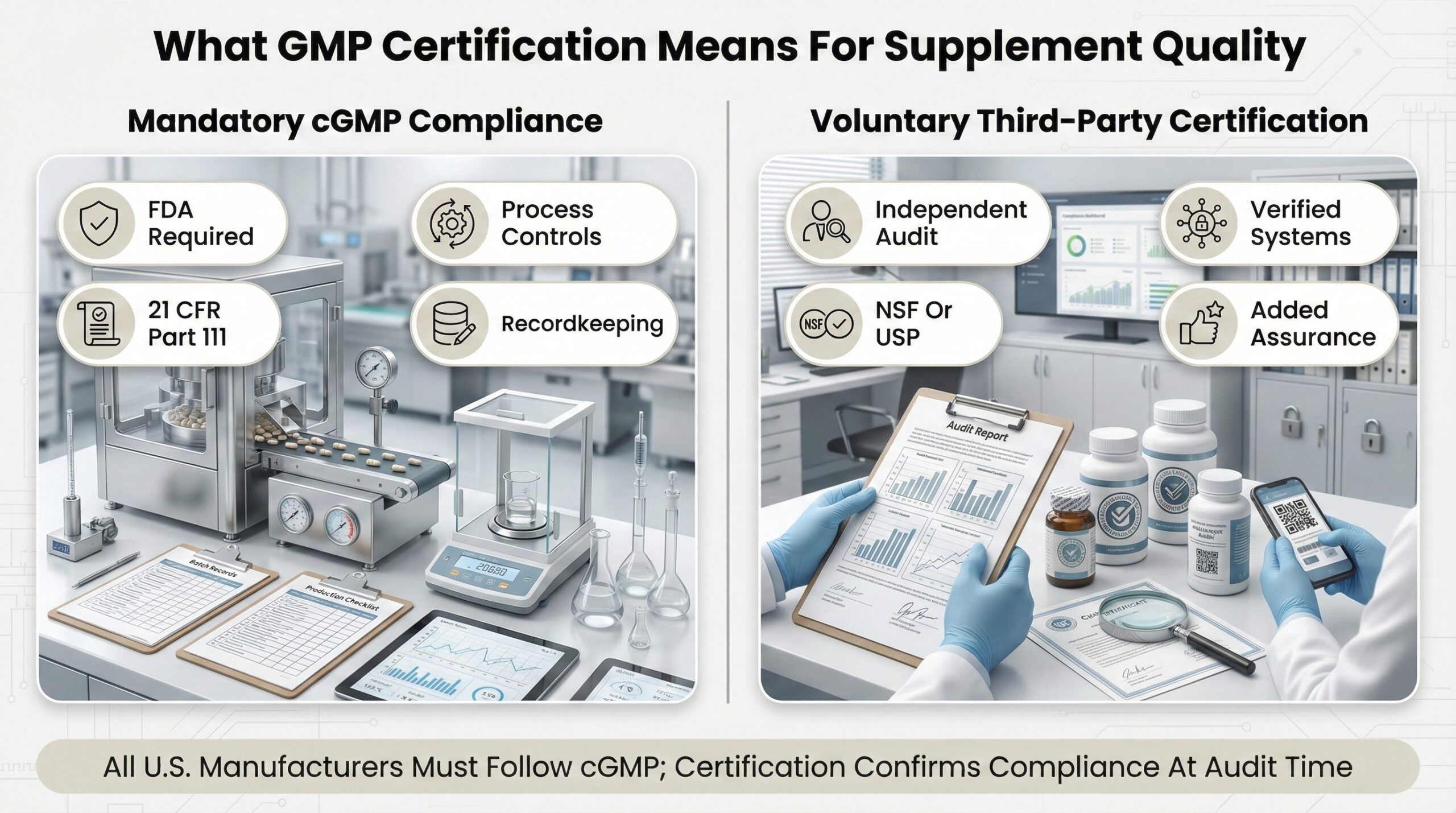
What GMP Certification Means for Supplement Quality
March 10, 2026
Why Peptide Capsules are Often Ineffective
March 10, 2026